Gender
specific factors associated with having stopped smoking among in-school
adolescents in Ukraine: results from the Global Youth Tobacco Survey 2005
Alice Hazemba, Seter
Siziya, Adamson S Muula, Emmanuel Rudatsikira
Abstract
Background: The prevalence
of cigarette smoking in Ukraine is different between genders and is among the
highest in the world. There is need to identify gender-specific factors that
are associated with having stopped smoking among adolescents.
Findings: We used
data from the Ukraine Global Youth Tobacco Survey 2005. We carried out a
backward stepwise logistic regression analysis with having stopped smoking as
the outcome. Altogether, 2800 adolescents reported having ever smoked
cigarettes. Overall 64.1% (63.4% male, and 65.5% female) adolescents reported
having stopped smoking. Male adolescents who stated that smoking decreases body
weight were 25% more likely, while female adolescents were 9% less likely to
stop smoking. While male adolescents who received support on how to stop
smoking from a family member were 7% less likely, female adolescents were 60%
more likely to stop smoking. Furthermore, while male adolescents who received a
lecture on the harmful effects of smoking were 10% less likely, female
adolescents were 9% more likely to stop smoking. Finally both male and female
adolescents who were sure or most probably that they would not smoke a
cigarette offered to them by their best friends were more likely, and those
adolescents who were sure that smoking is harmful to health were less likely to
stop smoking.
Conclusions: Our study
has identified some factors that are associated with having quit smoking that
are genderspecific.We believe public health programs targeting adolescent
smoking should consider these factors in their design and implementation of
gender sensitive interventions.
Background
The
prevalence of tobacco smoking in Ukraine is among
the highest in the world [1,2]. Furthermore, the age
of initiation is getting lower [3]. In the
Kiev Global Youth Tobacco survey conducted in 1999, 41% of 13 to 15 year old
in-school reported being current cigarette smokers [4,5]. The Health Belief Model (HBM) is a psychological model that
aims to explain and predict health-related behaviours. The model focuses on the
attitudes and beliefs of individuals [6,7]. One other aspect of the HBM is the
role of cues of action such as a lesson in school or a family member who
discusses the harmful effects of smoking with the adolescent. The HBM has been
partly used in predicting health behaviour, including smoking, among college
students [8]. We used this model to identify factors that we used in the analysis.
While the incidence and prevalence of smoking in Ukraine has been reported to
be growing [2], there are limited data on the cessation of smoking among
adolescents and more so on gender-specific correlates for stopping smoking. In
order to inform smoking prevention programs in Ukraine, we explored the
gender-specific correlates of self reported cessation of smoking among adolescents.
Methods
Study design and data collection
Our
study involved secondary analysis of cross sectional
data from the Ukraine Global School Youth Tobacco
Survey (GYTS) conducted in 2005. The GYTS uses a two-stage
probability sampling technique, in which schools are the primary sampling units
[9]. The core GTYS questionnaire was adapted to the Ukrainian needs and does
not match the core questionnaire.
Data analysis
Our
data analysis was restricted to smoking participants and those who had smoked cigarettes
but were no longer smokers. Data analysis was performed using SPSS version 14.0
software. A weighting factor was used in the analysis to reflect the likelihood
of sampling each student and to reduce bias by compensating for differing patterns
of non response. We obtained frequencies as estimation of prevalence of the
main outcome (ever having stopped smoking), and other descriptive
characteristics of the sample. We report unadjusted odds ratios (OR) from
bivariate analyses. We also conducted a backward stepwise logistic regression
analysis to estimate the associations between relevant predictor variables and
the outcome, and were port adjusted odd sratios (AOR) with their 95% confidence
intervals (CI) from this analysis.
Results
Data
on whether participants who had ever smoked but had stopped smoking cigarettes
or were still smokers were available from 2800 out of 7727 participants. Half (50.0%)
of the participants were males, and 35.5% of the respondents (35.7% of males,
and 35.4% of females) were of age 14 years. Overall, 60.6% of the participants (64.2%
males and 56.3% females) were current smokers and 64.3% of the adolescents
(63.4% of males, and 65.5% of females) reported having stopped smoking
cigarettes. The period since they stopped smoking varied from less than 1 month
to 3 years or more. Further description of the sample is shown in table 1.

Association of age with stopping smoking
Compared
to adolescents aged 15 years old and older, both male and female adolescents
who were of age less than 13 or were 14 years old were less likely to stop smoking,
while those who were of age 13 years were more likely to stop smoking
cigarettes (Table 2).

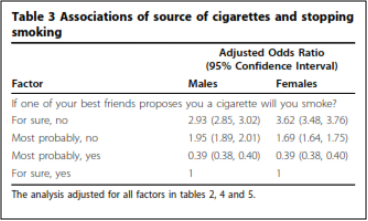
Best friend as source for cigarettes
Both
male and female adolescents who would definitely not accept an offer of a
cigarette from a close friend to Smoke it were more like lyto have stopped smoking
cigarettes compared to adolescents who would
definitely accept an offer of a cigarette from
a best friend and smoke it (AOR = 3.02 for
males and AOR = 3.62 for females) as shown in table 3.
Harmful effects of cigarette smoking
While
male adolescents who had a lecture in the previous year of the survey on
harmful effects of smoking were 10% (AOR = 0.90) less likely to have stopped smoking,
female adolescents were 9% (AOR = 1.09) more likely to have stopped smoking
compared to adolescents who did not have such a lecture. Male adolescents who
reported that cigarette smoking decreases body weight were 25% (AOR = 1.25)
more likely to stop smoking, while female adolescents were 9% (AOR = 0.90) less
likely to have stopped smoking compared to adolescents who said that cigarette
smoking did not affect body weight. Both male and female adolescents who
reported that cigarette smoking is definitely harmful to health were less
likely to stop smoking compared to adolescents who were most probably not
certain that smoking is harmful to health (AOR = 0.92 for males and AOR = 0.66
for females). Furthermore, both male and female adolescents who felt that
smoking increases boy weight were more likely to stop smoking (Table 4).

Sources of support or advice on how to stop smoking
Both
male and female adolescents who received support or advice on how to stop
smoking from a programme or professional were less likely to stop smoking (AOR
= 0.91 for males, and AOR = 0.93 for females), and while male adolescents who
received support or advice from a member of the family were less likely to stop
smoking (AOR = 0.93), female adolescents were more likely to stop smoking (AOR
= 1.60) compared to adolescents who had not ever received support or advice
(Table 5).

Discussion
Our
analysis of the Ukraine Global Youth Tobacco Survey 2005 has shown that, unlike
among adults [1], there was no gender difference in cigarette smoking. This finding
is consistent with previous reports which have indicated that there is no
gender difference in tobacco use in Europe and United States [10,11]. Using
data from repeat GYTS from 100 sites around the world, Warren et al report that
tobacco use among girls is likely increasing [12]. We first present a
discussion of factors associated with stopping smoking that were not significantly
different between gender, and then present factors associated with stopping
smoking that were different between gender.
Both
male and female adolescents who were younger were less likely to stop smoking
suggesting that this was the age group for experimenting smoking, and those not
in favour of the behaviour would have more likely stop smoking immediately.
Meanwhile, adolescents who would have continued to smoke would have been less likely
to stop smoking at a later age.
There
were no gender differences in smoking cessation
related to age, being offered a cigarette by a best
friend, weight increase, and getting support or advice
on how to stop smoking from a professional or friend.
Both male and female adolescents who were of age less
than 13 or of age 14 years, certain that cigarette
smoking is harmful to health, and had received
help on quitting smoking from a professional
or friend were less likely to have stopped
smoking than those who did not. Both male and
female adolescents who were of age 13, definitely would not/most probably would
not accept cigarettes from a peer, and perceived smoking increases body weight
were more likely to stop smoking. We believe this is important information that
public health policy makers and professionals involved in the designing and
delivery of interventions aimed to prevent adolescent smoking in Ukraine need
to consider in designing interventions that are not gendersensitive. It is
interesting to note that both male and female adolescents who reported that
they would definitely not accept a cigarette from a peer were more likely to
have stopped smoking that those who would not. One sense, this would suggest
that adolescents who are committed to no longer smoke were more successful to
have stopped smoking. Alternatively, our finding may suggest that adolescents
who have already quit smoking are more likely not to accept a cigarette from a peer
than those who are still smoking. Due to the cross sectional design of our
study, however, it is not possible to tease out which of the two explanations
may be more likely. It is however obvious that comparing adolescents who have
stopped smoking to those who are still smoking, those that have stopped smoking
reported that they would not accept a cigarette offer from a peer more than
those that are still smoking. Smoking cessation programs should seriously
consider the role of peers in facilitating continued smoking in adolescents who
may wish to quit.
We
found that both male and female adolescents who reported having received advice
on how to stop smoking from professionals or friends were less likely to stop smoking
suggesting that these sources may not have regarded as credible by the
adolescents; the reason partly being that some professionals also smoke cigarettes.
Findings from this study indicate that there were gender differences in smoking
cessation related to the perception of the effects of smoking on reducing body weight,
support or advice on how to stop smoking from a family member or lecture on the
harmful effects of smoking. Previous studies have reported gender differences in
responses to smoking cessation messages [13] as well as tobacco cessation
interventions [14,15].
We also assessed
whether the beliefs about the effect of smoking on weight was associated with
having quit smoking. In the GYT Ssurvey adolescentshad been asked whether they
thought that smoking was associated with weight gain or weight loss.
Adolescents who believed that smoking makes one’s weight decrease were more
likely to have stopped smoking among male adolescents, and less likely to have
stopped smoking among female adolescents. What does this mean in the context of
Ukraine? In many of the Western countries and lately in emerging economies,
female adolescents in general perceive themselves to be overweight or heavy.
Lean body weight is desirable. In many of these settings also, smoking is
perceived as resulting in lean body weight [16-18]. Some female adolescents
smoke in order to achieve or maintain a lean body weight [19,20]. Different perceptions
of body weight may be different between genders and may explain why male
adolescents were more likely to stop smoking in favour of a heavy body weight.
The
finding that while male adolescents who received support or advice from family
members were less likely to stop smoking, and female adolescents were more
likely to stop smoking suggest that female adolescents took family members as
credible source of information on cessation of smoking while male adolescents did
not.
We
found that having had a lecture on the harmful effects of smoking was
associated with having quit smoking. A meta-analysis of adolescent smoking cessation
programs reported by Sussman et al [21] suggested that programs that included a
motivation enhancement component, cognitive-behavioural techniques, and social influence
approaches were more likely to have been successful. These authors also reported
that higher quit rates were found in school-based clinic and classroom modalities
and in programs consisting of at least 5 quit sessions. This finding is
consistent with our finding among female adolescents who were more likely to
stop smoking after having had a lecture on harmful effects of smoking. Although
we do not have a description of the content, conduct, frequency and number of
lectures that had been delivered to adolescents who reported to have had a
lecture, it is still heartening to note that having had a lecture on the
harmful effects of smoking was associated with less likelihood of having to
quit smoking among male adolescents.
Limitations of the study
Due
to the cross sectional nature of the study, it is not possible to confirm
whether the factors that were identified as associated with having quit smoking
preceded or followed quitting. The study also relied on self-reported history
of having quit smoking. We did not verify that the adolescent had indeed quit
smoking, for instance by using biomarkers such as exhaled carbon monoxide. We also
did not have data on the nature of interventions that adolescents who reported
having received help from a health professional obtained. Furthermore, it is
unknown whether the adolescents who reported to have stopped smoking actually
purposefully stopped the behaviour or
just discontinued it.
Conclusions
We
have identified some factors that are associated with
having quit smoking that are gender-specific. We
suggest that adolescents’ smoking cessation programs
in Ukraine consider these factors in the design, implementation and evaluation
of their gender sensitive programs guided by the FCTC that Ukraine ratified in
2006.
References
1. Webb CP, Bromet EJ, Tintle NL, Schwartz JE, Gluzman SF,
Kostyuchenko S, Havenaar JM:
Smoking initiation
and nicotine dependence symptoms in Ukraine: Findings from the Ukraine World Mental Health
survey. Public Health 2007, 121:663-672.
2. Andreeva TI, Krasovsky KS: Changes in smoking prevalence in
Ukraine in 2001-2005. Tob Control 2007, 16:202-206.
3. Andreeva TI, Krasovsky KS: Correlates of smoking initiation
among young adults in Ukraine: a cross sectional study. BMC Public Health 2007,
7:106.
4. Kiev Global Youth
Tobacco Survey Fact Sheet. http
://www.aahperd.org/iejhe/2003_first/files/hill_2.html.
5. Warren CW, Riley L, Asma S, Eriksen MP, Green L, Blanton C, Loo
C, Batchelor S, Yach D: Tobacco use by youth: a surveillance report from the
Global Youth Tobacco Survey project. Bull World Health Organ 2000, 78:868-876.
6. Glanz K, Rimer BK, Lewis FM: Health Behavior and Health
Education. Theory, Research and Practice San Fransisco: Wiley & Sons 2002.
7. Glanz K, Marcus Lewis F, Rimer BK: Theory at a glance: a guide
for health promotion practice Bethesda: National Institute of Health 1997.
8. Von Ah D, Ebert S, Ngamvitroj A, Park N, Kang DH: Predictors of
health behaviours in college students. J Adv Nurs 2004, 48:463-474.
9. Centers for Disease Control and Prevention (CDC): Global Youth
Tobacco Surveillance, 2000-2007. Surveillance summaries, January 25 MMWR 2008, 57(No.
SS-1).
10. Rudatsikira E, Muula AS, Siziya S: Current cigarette smoking
among inschool American youth: results from the 2004 National Youth Tobacco Survey.
Int J Equity Health 2009, 8:10.
11. Rachiotis G, Muula AS, Rudatsikira E, Siziya S, Kyrlesi A,
Gourgoulianis K, Hadjichristodoulou C: Factors associated with adolescent
cigarette smoking in Greece: Results from a cross-sectional study (GYTS study).
BMC Public Health 2008, 8:313.
12. Warren CW, Lea V, Lee nr, McKenna M: Change in tobacco use
among 13-15 year olds between 1999 and 2008: findings from the Global Youth Tobacco
Survey. Glob Health Promot 2009, 16(Suppl):38-40.
13. Toll BA, Salovey P, O’Malley SS, Mazure CM, Latimer A, McKee
SA: Message framing for smoking cessation: the interaction of risk and gender. Nicotine
Tob Res 2008, 10:195-200.
14. Anthenelli RM, Blom TJ, McElroy SL, Keck PE Jr: Preliminary
evidence for gender-specific effects of topiramate aid to smoking cessation.
Addiction 2008, 103:687-694.
15. Levin RF, Stout JM, Singleton JK, Londrigan M, Feldman HR,
McMillan E: Gender’s
effect on the efficacy of smoking cessation interventions. Nurs Times 2004, 100:32-34.
16. Cheung PC, Ip PL, Lam ST, Bibby H: A study on body weight
perception and weight control behaviours among adolescents in Hong Kong. Hong Kong
Med J 2007, 13:16-21.
17. Forman-Hoffman V: High prevalence of abnormal eating and
weight control practices among
U.S. high-school students. Eat Behav 2004, 5:325-336.
18. Flanagan JR, Bandomir CA: Coming to grips with weight
perception: effects of grasp configuration on perceived heaviness. Percept
Psychophys 2000, 62:1204-1219.
19. Dowdell EB, Santucci ME: Health risk behavior assessment:
nutrition, weight, and tobacco use in one urban seventh-grade class. Public
Health Nurs 2004, 21:128-136.
20. Winter AL, de Guia NA, Ferrence R, Cohen JE: The relationship
between body weight perceptions, weight control behaviours and smoking status among
adolescents. Can J Public Health 2002, 93:362-365.
21. Sussman S, Sun P, Dent CW: A meta-analysis of teen cigarette
smoking cessation. Health Psychol 2006, 25:549-557.
Referensi :
1.
http://link.springer.com/article/10.1186/1756-0500-3-76/fulltext.html
Tidak ada komentar:
Posting Komentar